High Risk Antibiotics
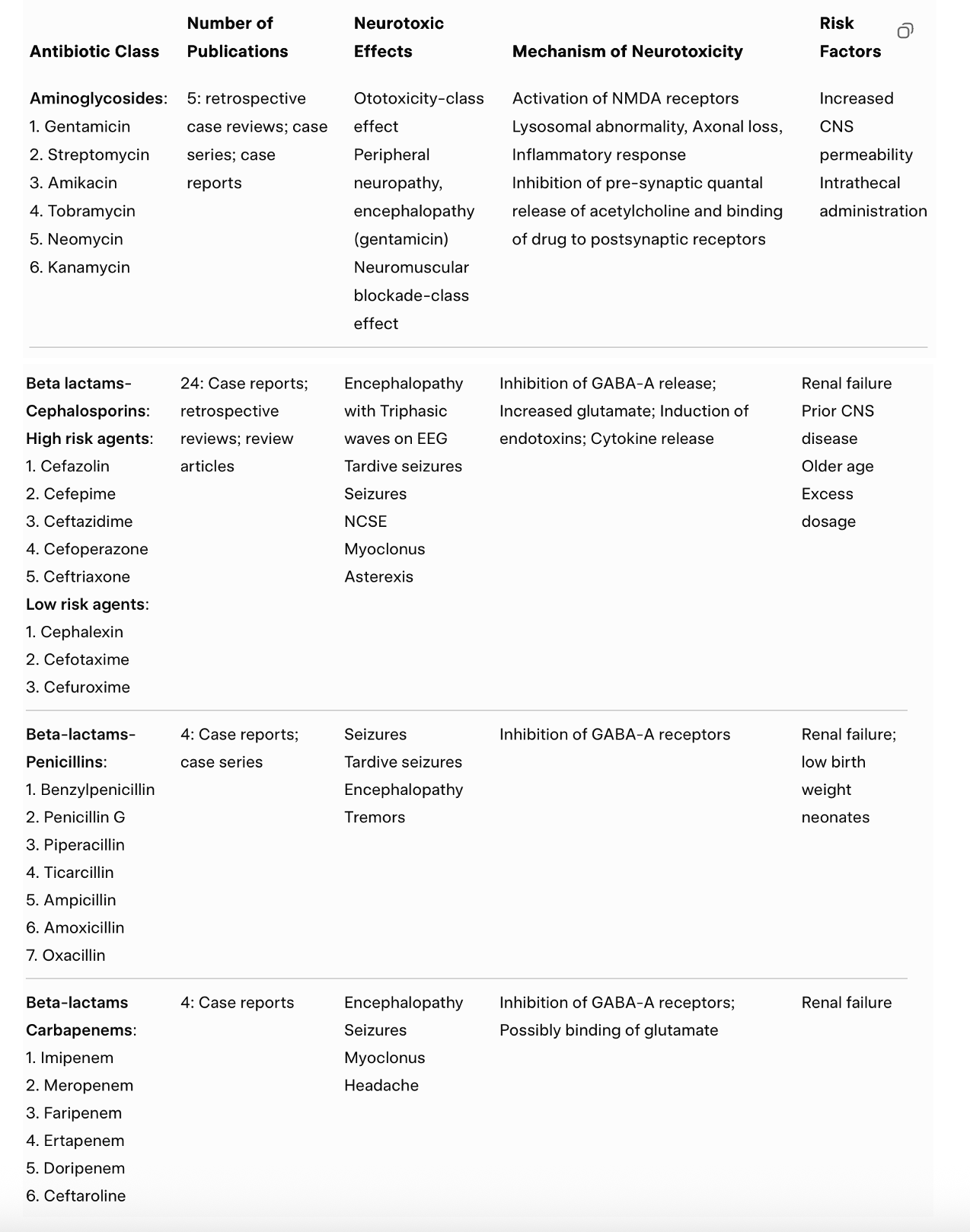
Fluoroquinolones (e.g., ciprofloxacin, levofloxacin, moxifloxacin, ofloxacin) are broad-spectrum antibiotics that kill bacteria by blocking DNA gyrase and topoisomerase IV, enzymes bacteria need to replicate and repair DNA (1). Because they’re potent and penetrate many tissues, regulators recommend reserving them for situations where benefits clearly outweigh risks, especially when safer alternatives exist (1).
A key reason they’re viewed as “high-risk” in sensitive people is their neurologic/psychiatric side-effect profile. Mechanistically, fluoroquinolone neurotoxicity is linked to CNS excitation, including GABA-A receptor inhibition/antagonism (reducing the brain’s main inhibitory brake) and effects that can increase excitatory signaling (often discussed alongside NMDA activation) (1 & 2). Clinically and in FDA safety communications/labeling, reported CNS effects include anxiety, agitation, insomnia, confusion/delirium, hallucinations, depression, suicidal thoughts, and seizures in some cases; the FDA has specifically warned to stop the drug if serious CNS/psychiatric effects occur (1).
Doxycycline is a tetracycline antibiotic used for acne, respiratory infections, tick-borne illnesses, and malaria prophylaxis. Its primary antibacterial mechanism is blocking bacterial protein synthesis by binding the 30S ribosomal subunit. Even though it’s “just an antibiotic,” official labeling and clinical reporting include notable CNS/psychiatric adverse effects in some people (e.g., anxiety, depression, insomnia, abnormal dreams, hallucinations, suicidal ideation) as post-approval reactions (5).
On the serotonin/SSRI-like angle: psychiatrist David Healy argues that doxycycline has serotonin reuptake–inhibiting properties and that, in susceptible individuals, it can produce agitation/toxic behavioral states that can resemble SSRI activation—he even notes that people who become agitated on SSRIs may also become agitated on doxycycline (and vice versa) (3). Separately (and more conservatively), there is published clinical literature describing severe mood/behavioral reactions temporally linked to doxycycline, including a BMJ Case Reports series of suicidal ideation(with two deaths) that improved with discontinuation in some cases (4). For a PFS/PSSD/PAS audience, the careful takeaway to communicate is: some people report doxycycline can destabilize them, and one proposed explanation (not universally accepted) is serotonin-system involvement, while another is broader CNS toxicity; either way, it’s a “proceed cautiously” item for sensitive individuals (5).
(2) https://pmc.ncbi.nlm.nih.gov/articles/PMC10957204/
(3) https://davidhealy.org/doxycycline-and-stephen-oneill/
(4) https://pubmed.ncbi.nlm.nih.gov/24347450/
(5) https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/205931s006%2C208253s004lbl.pdf
Crash Anecdotes:
https://ncmedsoc.org/do-you-know-what-floxing-is-could-it-be-deadly-to-your-patients/
https://www.reddit.com/r/PSSD/comments/10jfcnv/did_doxycycline_antibiotic_crash_you_or_help_you/
https://www.reddit.com/r/PSSD/comments/16pfrhe/doxycycline_is_causing_me_anxiety_is_it_safe_to/
https://www.reddit.com/r/PSSD/comments/18jzuv3/crash_from_doxycycline/
My Personal Risk Ranking:
High Risk of Permanent Worsening (for PFS/PSSD/PAS):
If you currently have PFS/PSSD/PAS, these substances may carry an high risk of worsening symptoms—potentially in a lasting way—and is best avoided. Other antibiotic classes if available may be a risk mitigation strategy.