Ashwaganda
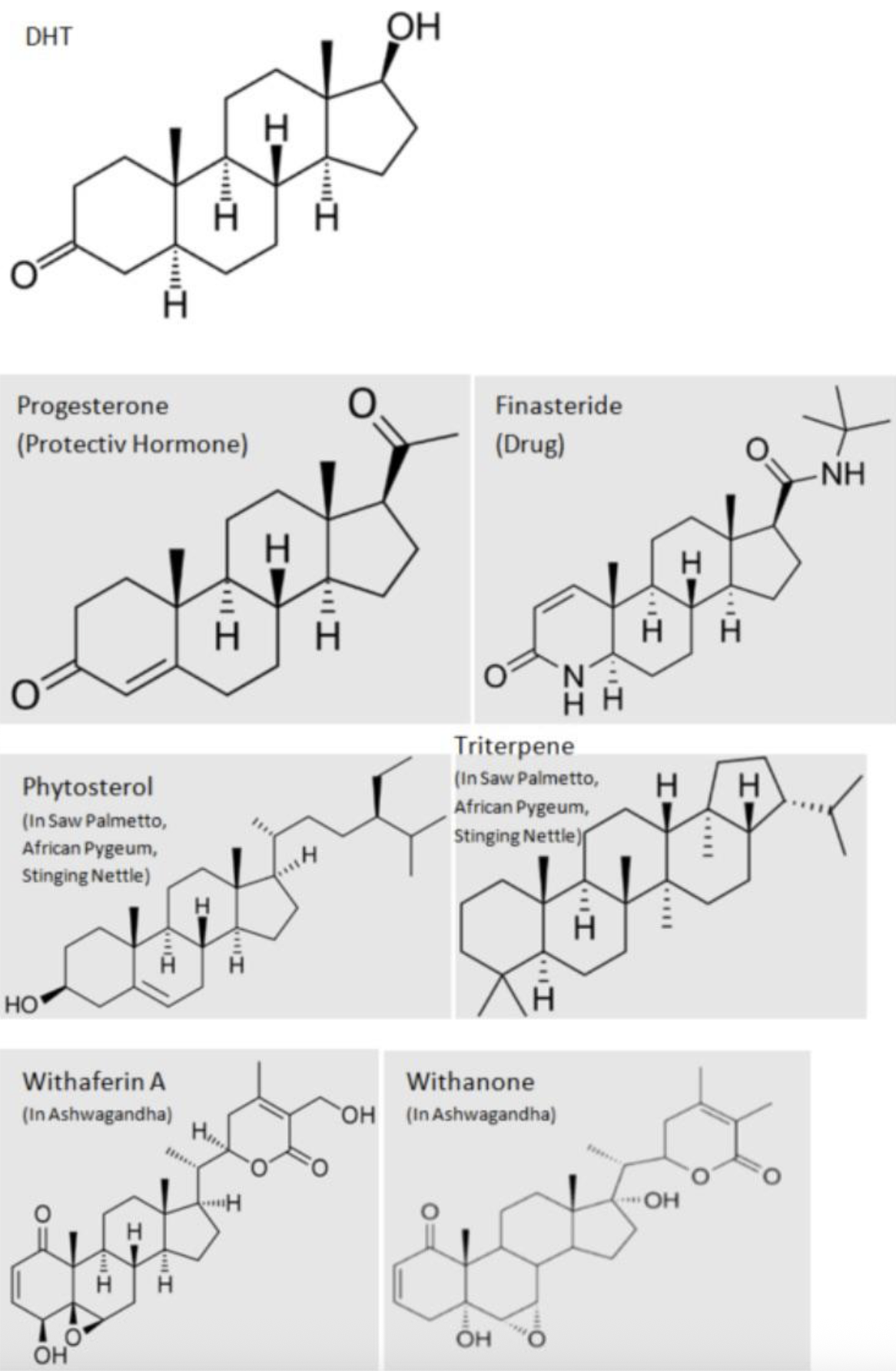
Ashwagandha (Withania somnifera) is often promoted as a testosterone-boosting “adaptogen,” but some users report side effects that resemble those associated with 5-alpha-reductase inhibitors (5-ARIs) like finasteride and saw palmetto—most notably sexual dysfunction and anhedonia/emotional blunting. One proposed explanation is that certain compounds in ashwagandha may overlap with anti-androgen / 5-alpha-reductase–related pathways, though the strength and real-world significance of this effect isn’t settled and likely varies by extract and dose.
It’s also important to understand the hormone logic people cite: blocking 5-alpha-reductase reduces conversion of testosterone → DHT, which can lead to higher testosterone but lower DHT. So “higher testosterone” does not automatically mean “more androgenic signaling overall,” especially if DHT-driven signaling is reduced. Because many people with PFS/PSSD/PAS appear unusually sensitive to shifts in androgen signaling and neurosteroid balance, ashwagandha is treated by many as a extreme-risk herb, particularly if someone has previously reacted to finasteride/saw palmetto or already has a fragile baseline.
Crash Anecdotes:
https://www.reddit.com/r/PSSD/comments/1ha0pky/has_anyone_else_experienced_an_ashwaganda_crash/
My Personal Risk Ranking:
Extreme Risk of Permanent Worsening (for PFS/PSSD/PAS):
If you currently have PFS/PSSD/PAS, this substance may carry an extreme risk of worsening symptoms—potentially in a lasting way—and is best avoided.
For those without these conditions, there are reports of a “post–ashwaganda syndrome” that can resemble PFS/PSSD/PAS although much less frequent for this over the counter supplement. Given the uncertainty and the potential severity of outcomes, the risk may not be worth the advertised benefits.